
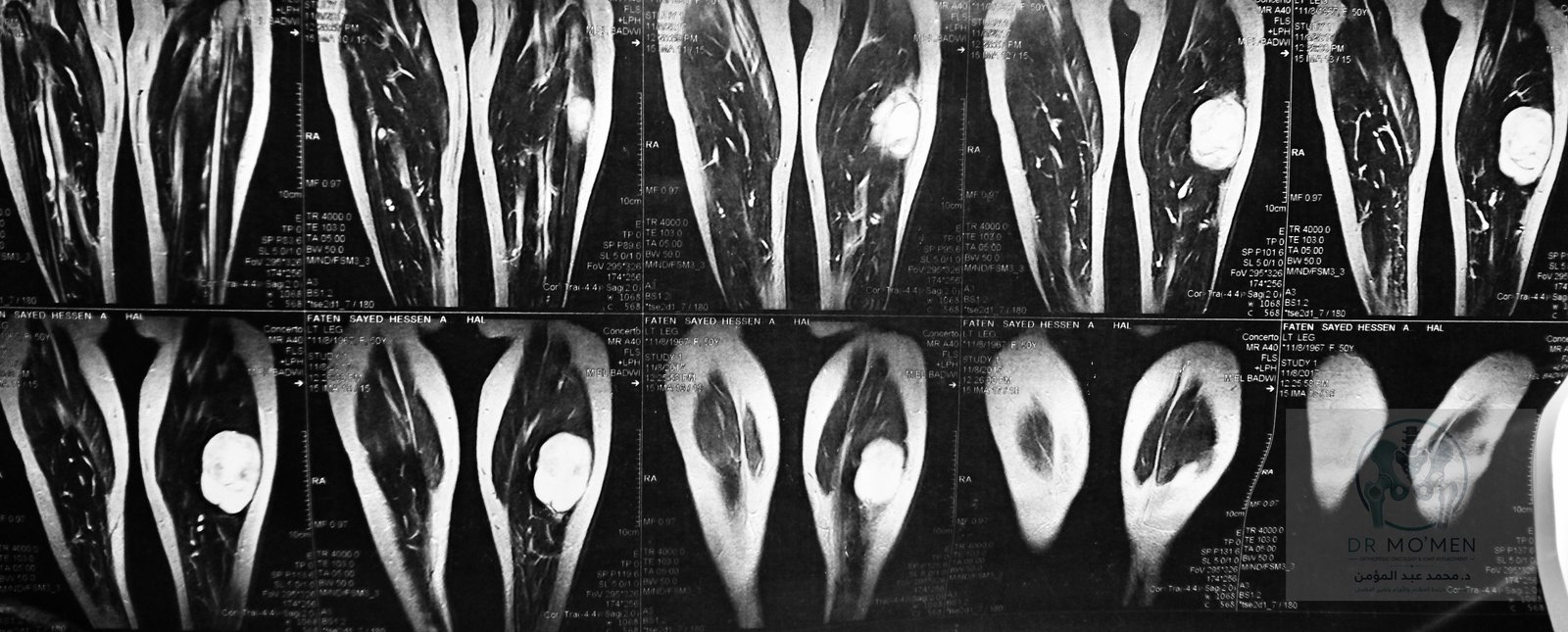
A deep posterior calf mass appeared sharply circumscribed on MRI and deceptively benign at surgery. Final histopathology instead confirmed high-grade myxoid liposarcoma with a round-cell component exceeding 25%.
Related specialist resources
Case summary
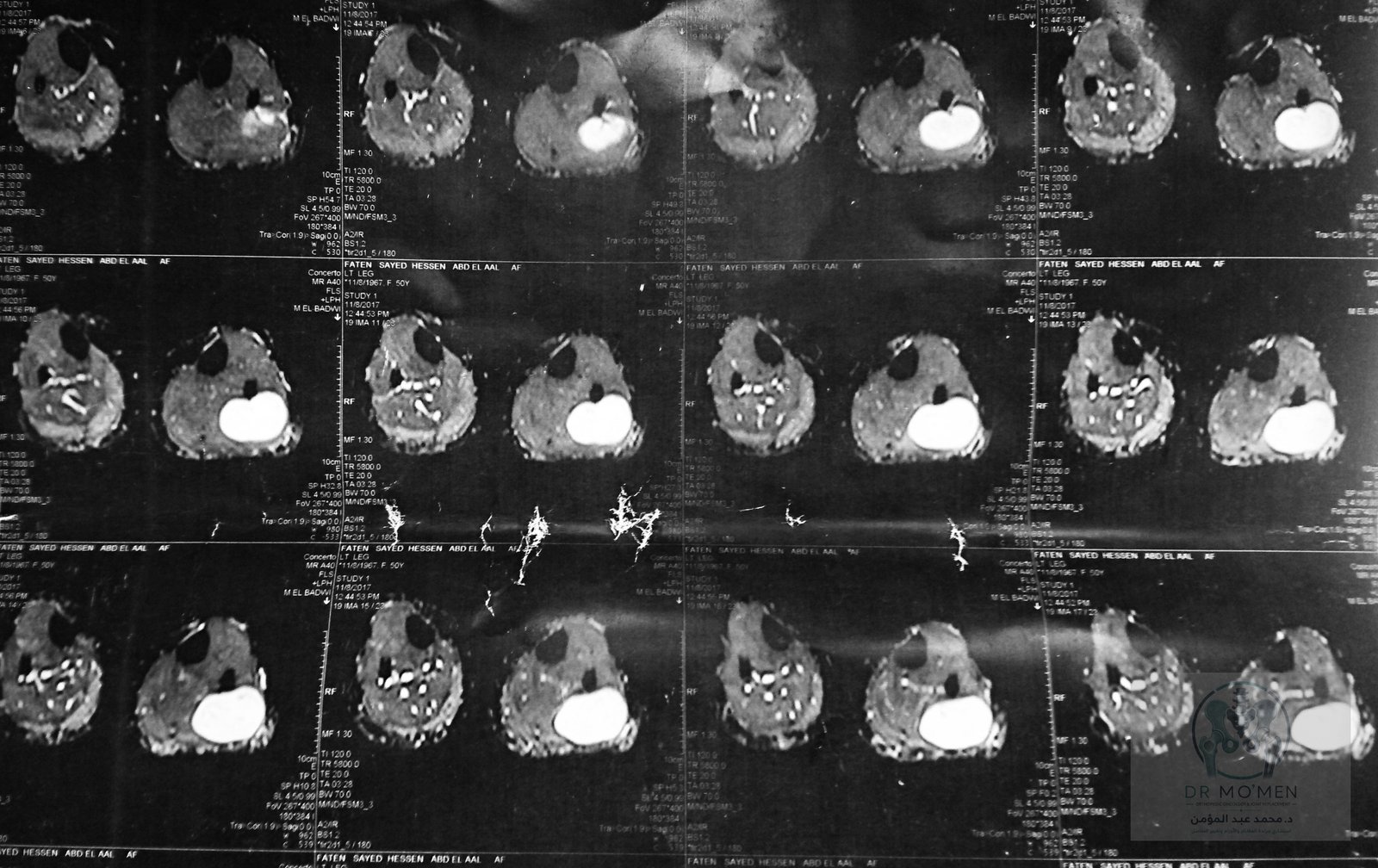
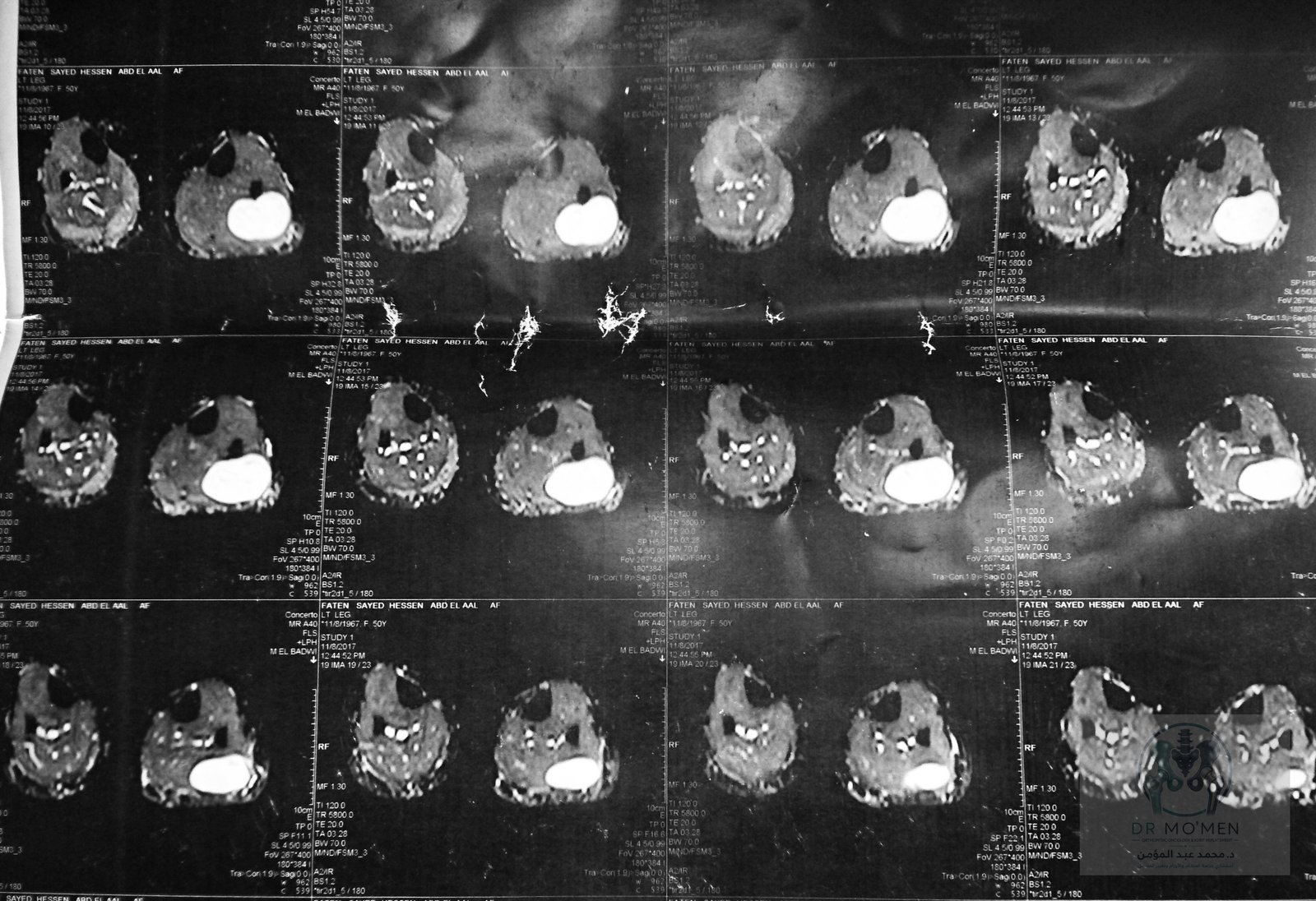
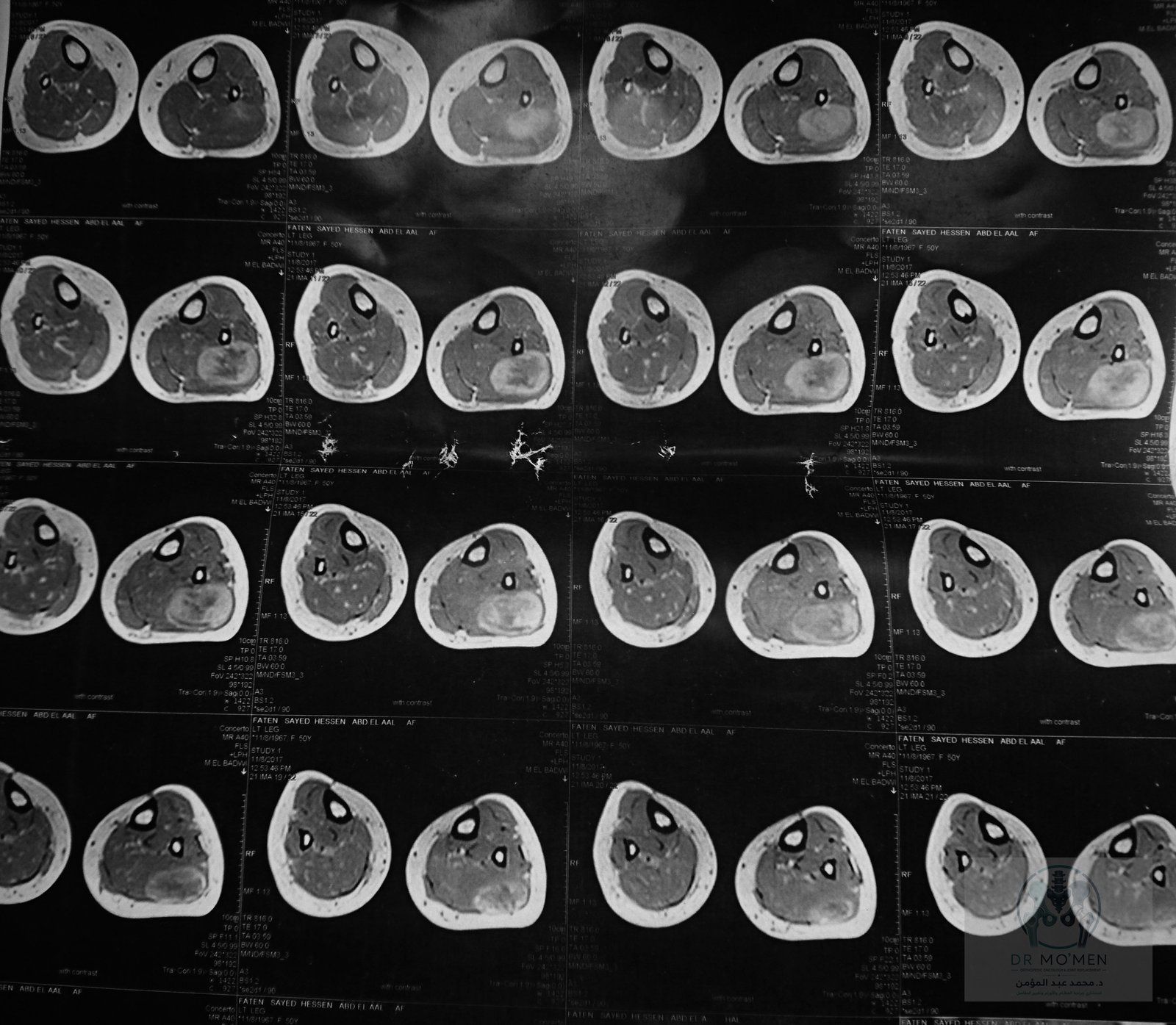
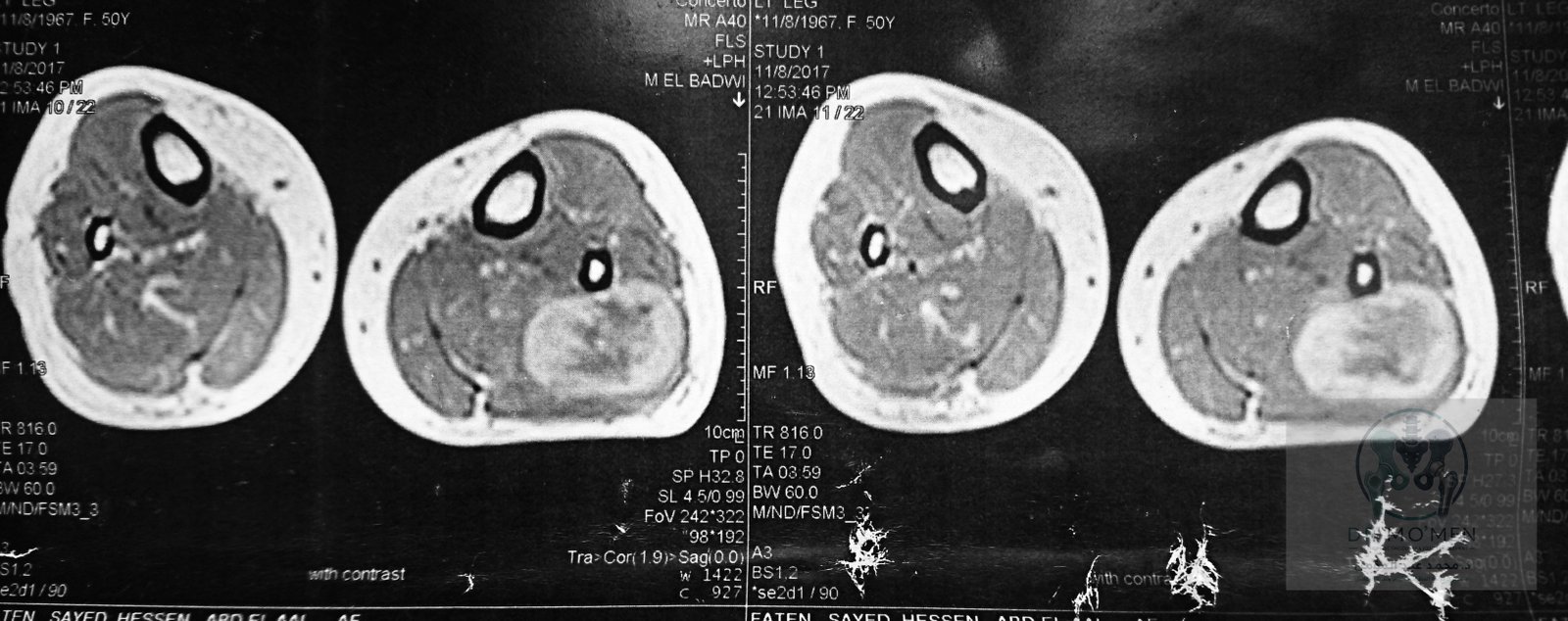
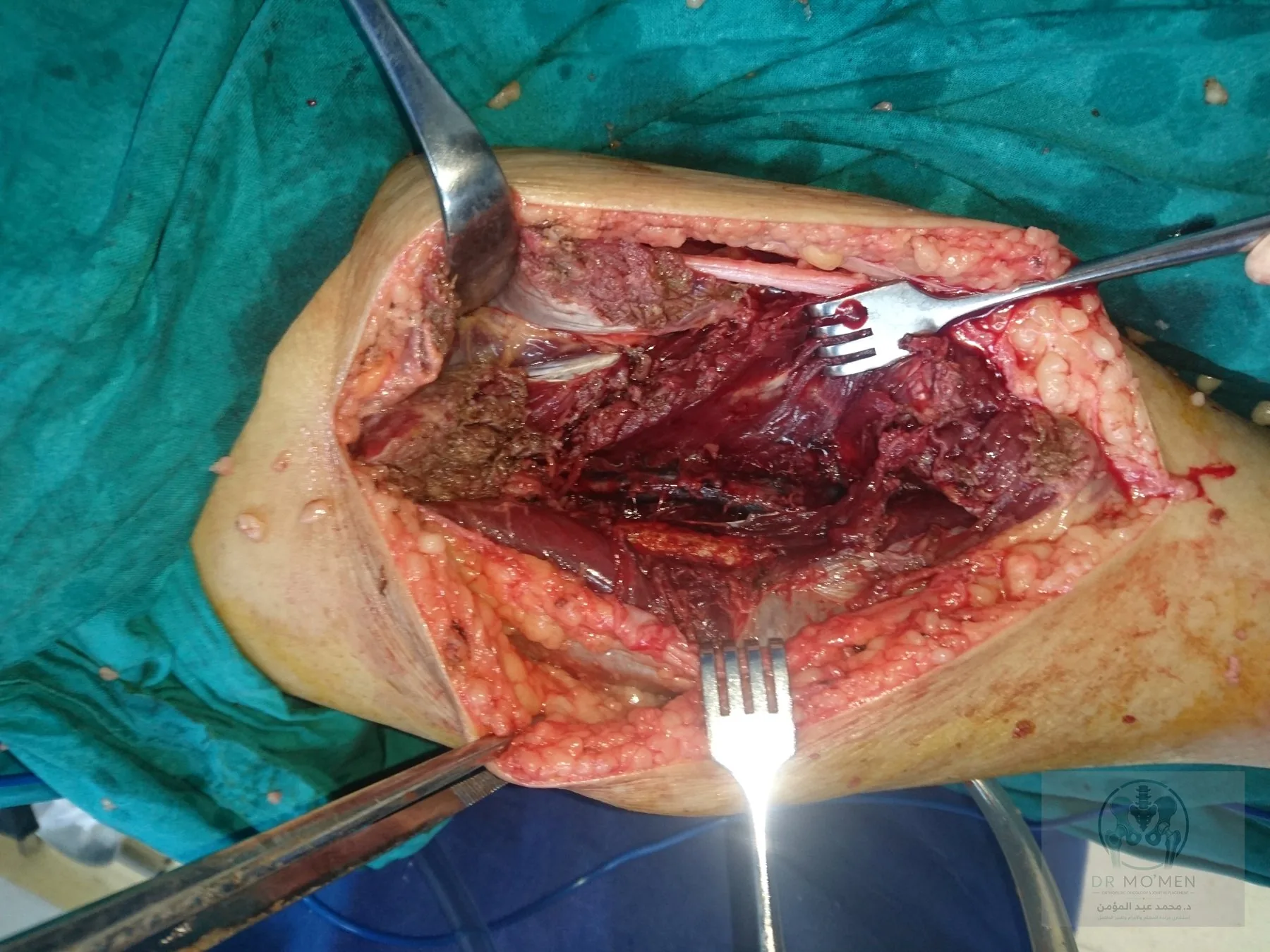
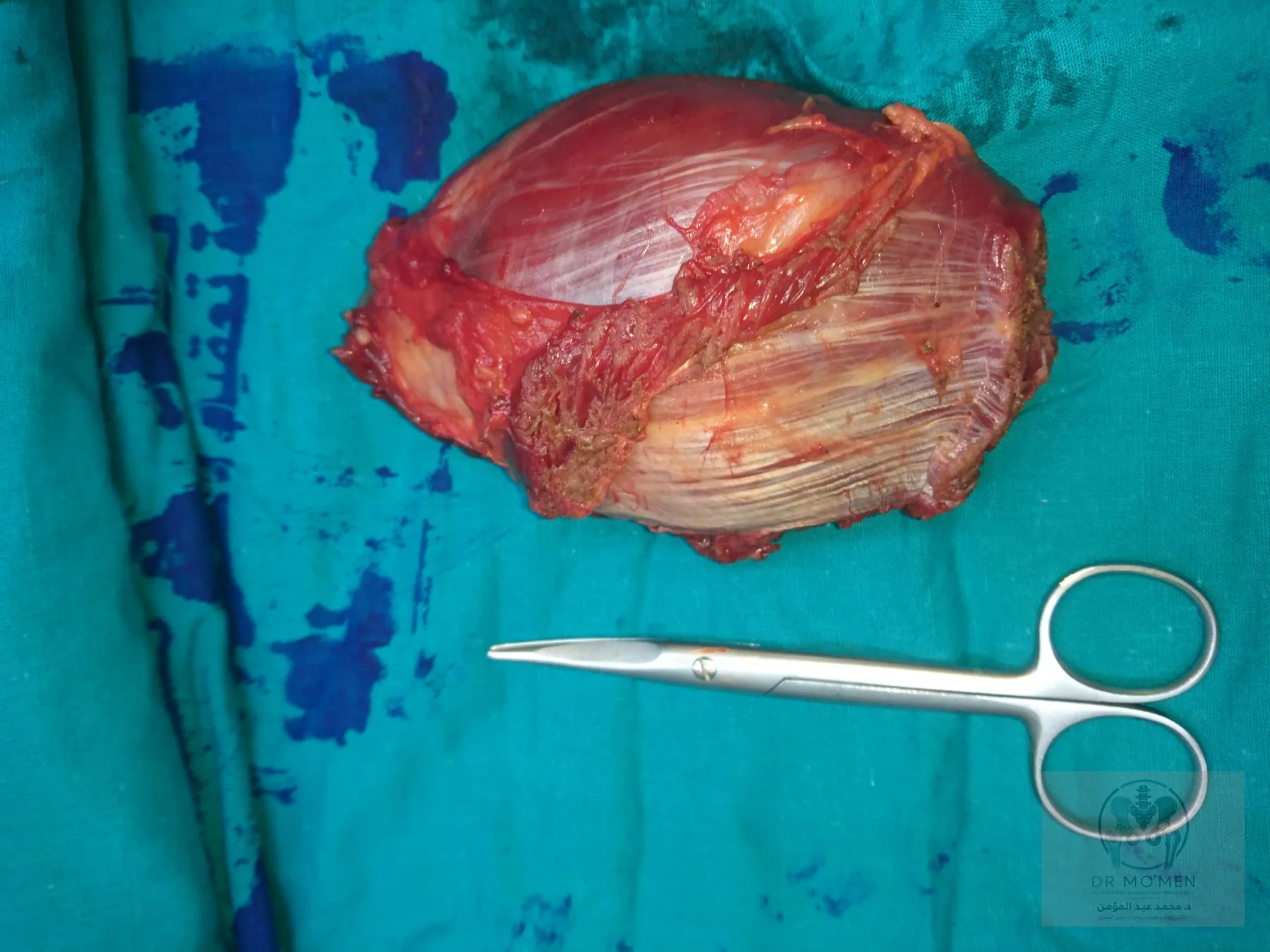
MRI demonstrated a well-circumscribed ovoid lesion with very high signal on fluid-sensitive sequences, strong post-contrast enhancement, and no bone involvement. The lesion was close to a neurovascular plane. At surgery it appeared smooth, glistening, and apparently encapsulated, with a distinct dissection plane. These features raised the possibility of a benign peripheral nerve sheath tumor, particularly schwannoma.
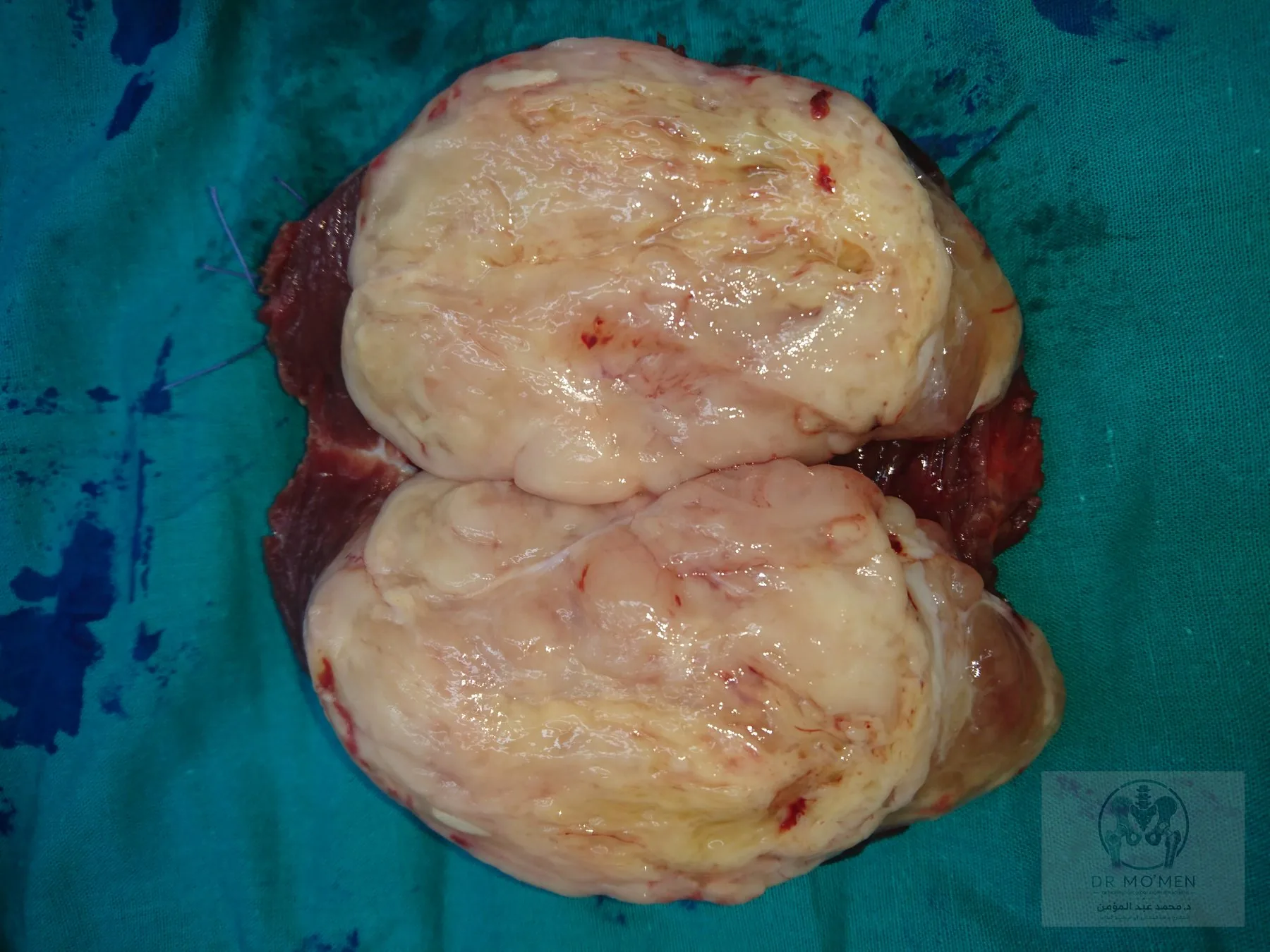
Final histopathology overturned that impression: high-grade myxoid liposarcoma with a round-cell component exceeding 25%, focal necrosis, and focal minimal muscle invasion. The closest reported surgical margin was approximately 1 mm anteriorly. The lateral aspect showed focal minimal tumor encroachment on the capsule without a cuff of peritumoral soft tissue; the posterior, medial, inferior, and superior margins were reported clear.
The diagnostic trap
Myxoid liposarcoma contains abundant water-rich myxoid matrix and may therefore appear bright, homogeneous, or pseudocystic on MRI. A smooth border, capsule-like surface, or clean operative plane does not establish benign biological behavior.
- A sharply circumscribed mass may still be malignant.
- A bright T2 lesion is not automatically a cyst, myxoma, or schwannoma.
- A pseudocapsule may not provide an oncologically adequate margin.
- Microscopic extension can exist beyond the visible tumor boundary.
What the pathology changes
Round-cell component above 25%
The round-cell component is an important adverse histologic feature in myxoid liposarcoma. A component exceeding 25% represents a substantial high-grade component, but prognosis still depends on stage, tumor size and depth, anatomical site, margins, metastases, and the complete specialist pathology review.
Margin interpretation
A close margin is not automatically synonymous with a microscopically positive margin. Exact R0/R1 classification requires review of the inked specimen, orientation, and pathology map. Nevertheless, a capsule-only or approximately 1 mm margin after an unplanned excision requires specialist reassessment.
Evidence-based pathway after an unexpected sarcoma diagnosis
- Specialist pathology review, including grade, round-cell proportion, necrosis, invasion, and mapped margins.
- Dedicated postoperative MRI of the surgical bed to assess residual disease and plan local treatment.
- Systemic staging including chest imaging; broader staging should be considered in a sarcoma center because myxoid liposarcoma may metastasize to extrapulmonary soft tissue and bone.
- Sarcoma multidisciplinary-team review to sequence surgery, radiotherapy, and any systemic treatment.
- Consideration of tumor-bed re-excision when margins can be meaningfully improved with acceptable morbidity.
- Individualized radiotherapy and systemic-therapy decisions; neither is automatic for every localized case.
- Long-term surveillance for local recurrence and the characteristic metastatic pattern.
Clinical and operative documentation




Core learning points
- Final pathology can overturn a plausible imaging and operative diagnosis.
- Deep adult soft-tissue masses require oncologic planning even when smooth, mobile, or apparently encapsulated.
- Myxoid matrix can produce a deceptively homogeneous MRI appearance.
- A >25% round-cell component is a substantial high-grade feature.
- Unexpected sarcoma after excision requires specialist pathology review, postoperative MRI, systemic staging, and MDT planning.
Frequently asked questions
Can a sarcoma look encapsulated?
Yes. Some sarcomas can be sharply circumscribed and appear to have a capsule or pseudocapsule; this does not exclude microscopic extension.
Why was MRI not enough?
MRI defines anatomy and tissue characteristics, but different tumors overlap in appearance. Definitive diagnosis requires appropriately planned tissue assessment.
What does a >25% round-cell component mean?
It indicates a substantial higher-grade cellular component and is an adverse feature, interpreted alongside stage, size, depth, margins, and metastases.
Is repeat surgery always mandatory?
No. Tumor-bed re-excision is considered when it can meaningfully improve margins with acceptable morbidity, based on MRI, pathology, anatomy, radiotherapy options, and MDT judgment.
Need specialist review of a soft-tissue tumor?
Send the original MRI, pathology report, and operative details for guidance on clinic or online review.
Book via WhatsApp