
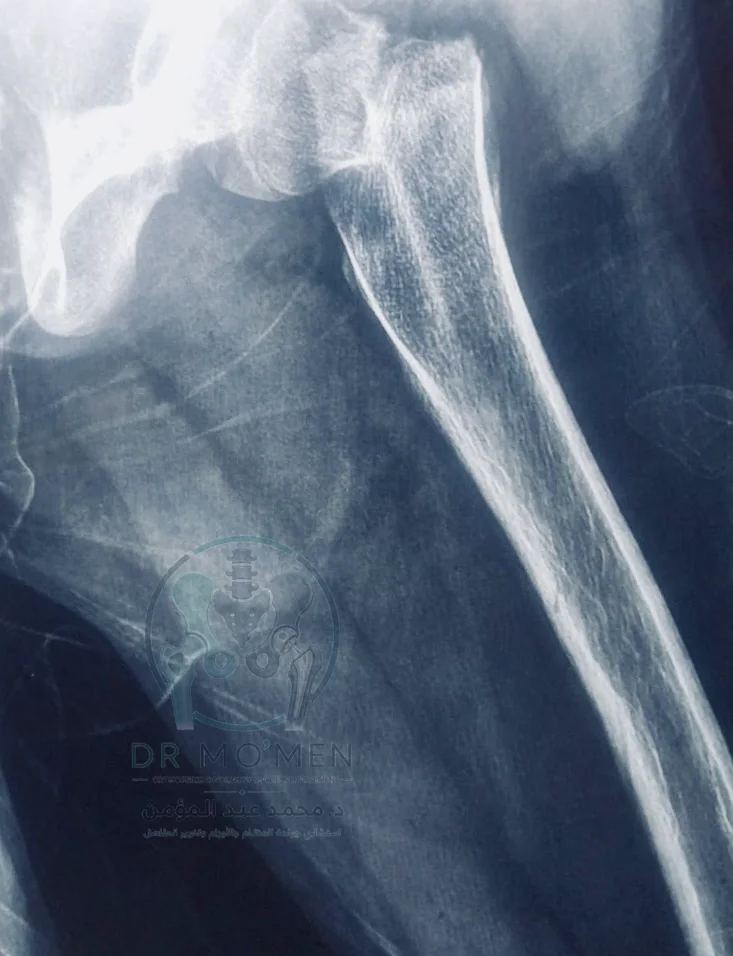
A 10-year-old girl presented after trauma with a displaced femoral neck fracture. Although the injury occurred during Eid al-Adha, the case required urgent assessment and surgical management because pediatric femoral neck fractures involve a sensitive anatomical region close to the blood supply of the femoral head.
Related pages
Why Pediatric Femoral Neck Fractures Require Careful Management
The femoral neck is close to the femoral head and its vascular supply. For that reason, displaced femoral neck fractures in children are not treated as simple fractures. Delayed or inadequate reduction may increase the risk of loss of reduction, nonunion, coxa vara, or femoral head complications.
The main objective is to restore anatomical alignment and provide stable fixation while preserving the hip joint as much as possible, with structured follow-up after surgery.
Surgical Management
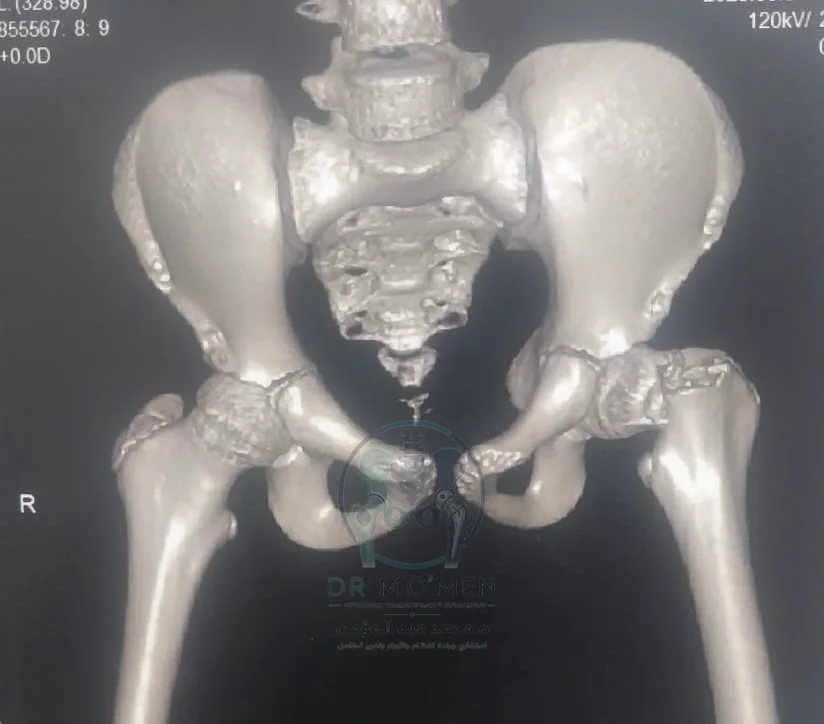
- Fracture evaluation using plain radiographs and 3D CT reconstruction to define the displacement pattern and plan fixation.
- Reduction of the femoral neck fracture under imaging control in the operating room.
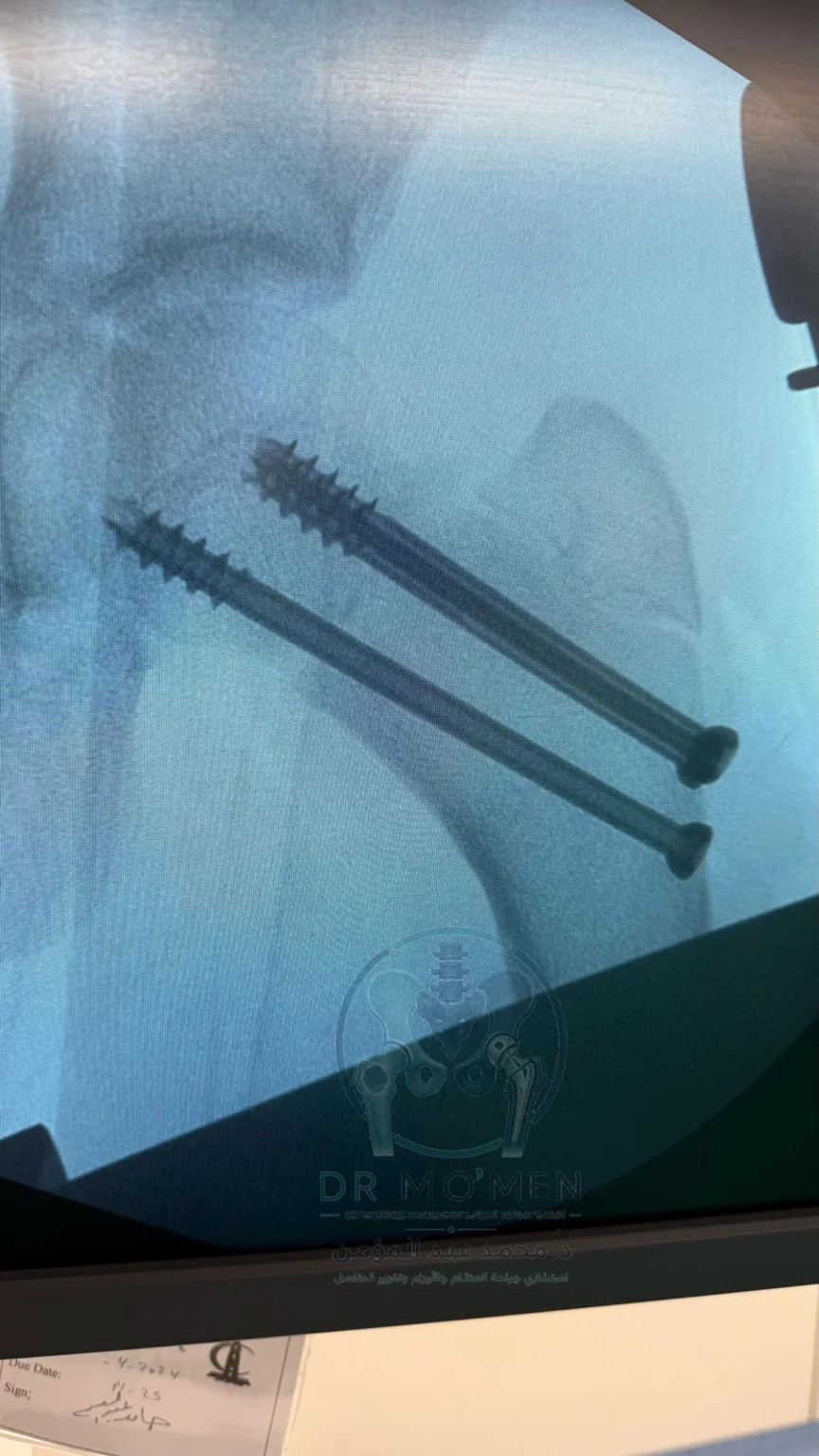
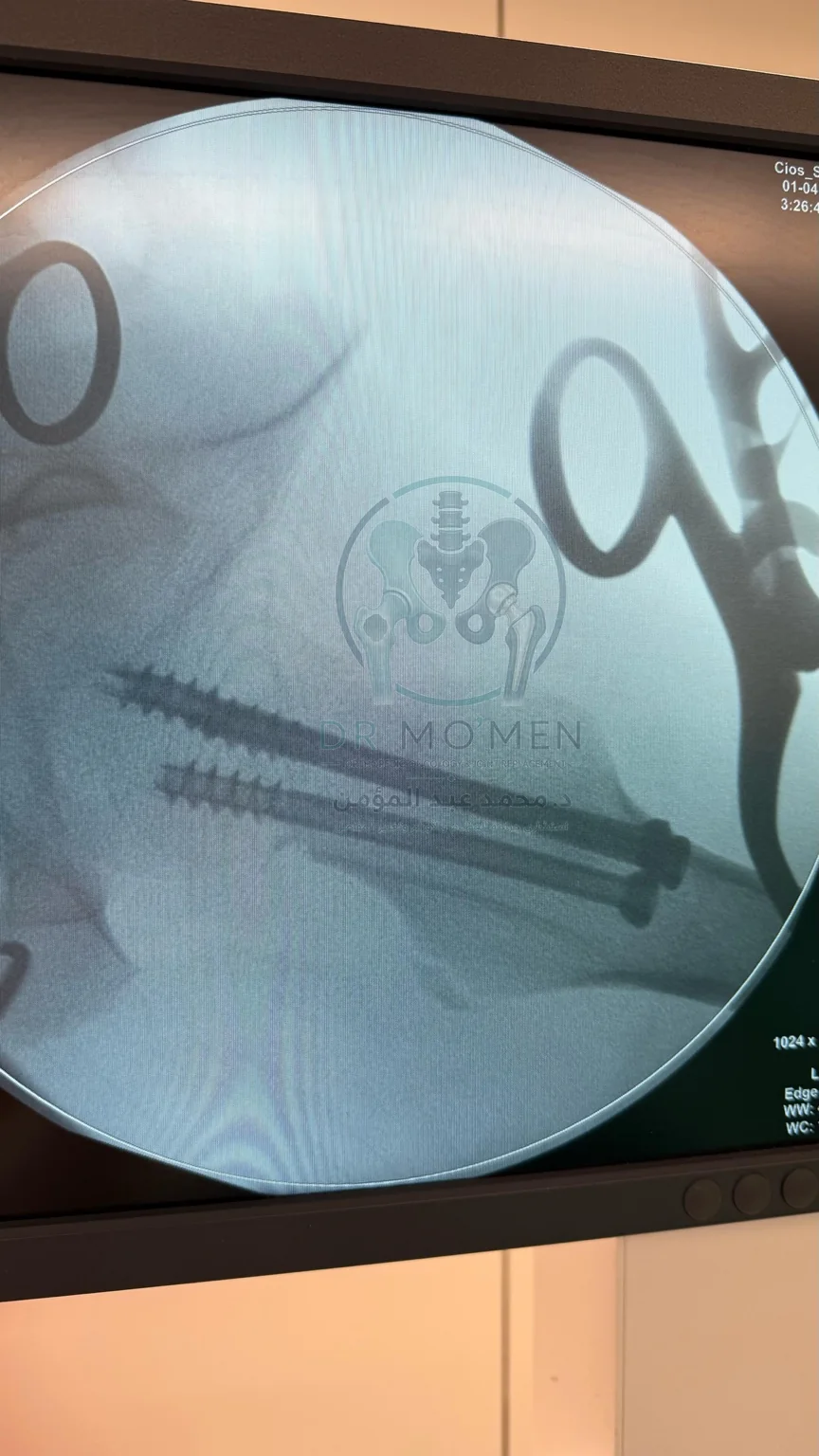
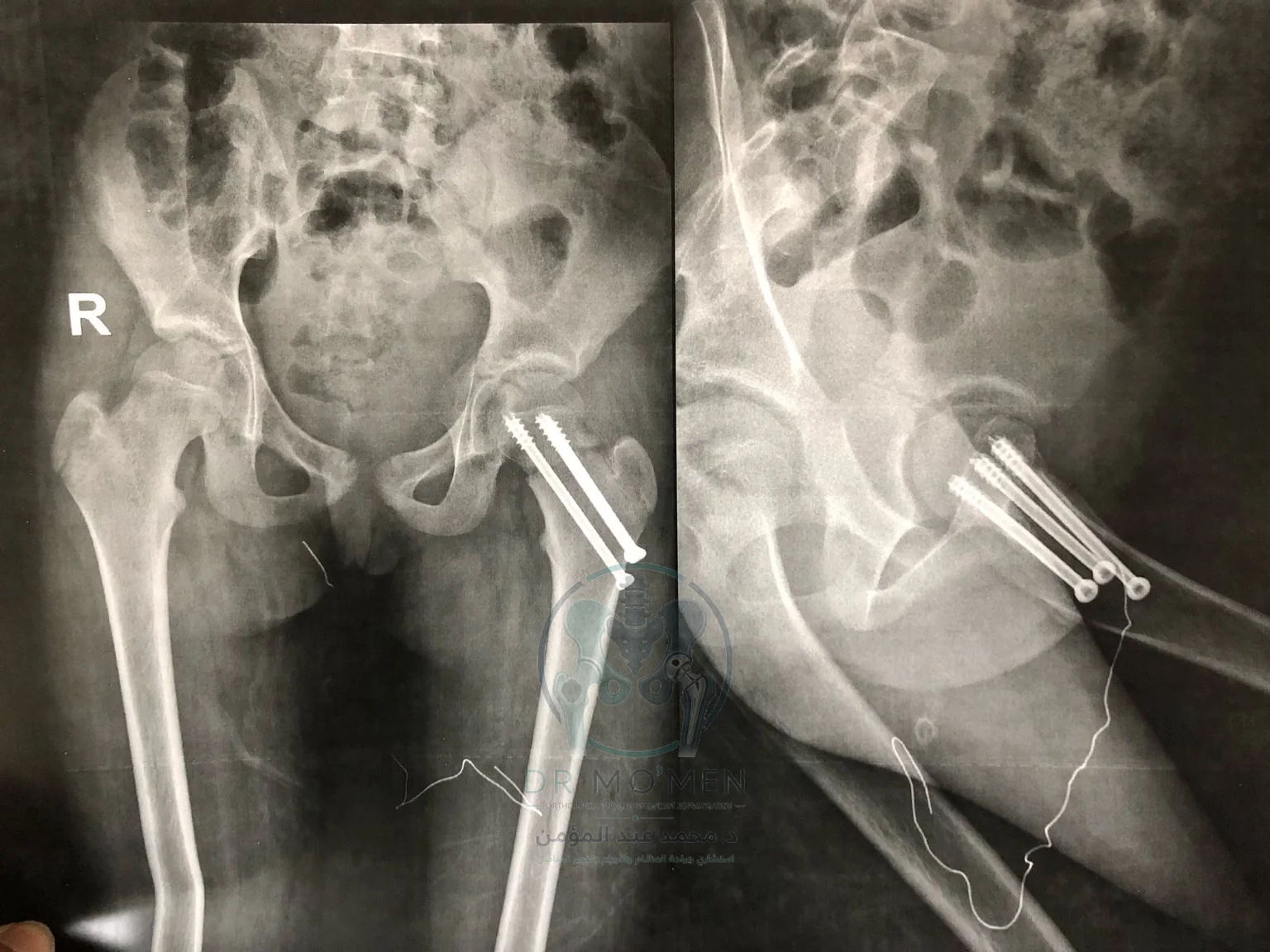
- Internal fixation using multiple cannulated screws with fluoroscopic confirmation in more than one view.
- Individualized postoperative weight-bearing and follow-up according to fixation stability and radiographic healing.
Follow-Up Result
Immediate postoperative radiographs showed acceptable screw position and stable fixation. At the 6-month follow-up, the radiographs showed maintained fixation with a reassuring appearance regarding alignment and healing in the available images.
Long-term follow-up remains important in pediatric femoral neck fractures to monitor hip development, femoral head viability, limb length, and potential late complications.
Radiographic Documentation
The following images are de-identified and watermarked for educational case-library use.



Patient-Facing Summary
A femoral neck fracture in a child is uncommon but clinically important. Successful management depends on rapid evaluation, accurate reduction, stable fixation, and structured follow-up after surgery. This case demonstrates the importance of timely surgical decision-making when a pediatric hip fracture is displaced and anatomically sensitive.
Patient FAQ
Is a femoral neck fracture in a child serious?
Yes. It is an uncommon but important injury because the fracture is close to the femoral head and its blood supply. Displaced fractures should be assessed urgently by a specialist.
Why were cannulated screws used?
Cannulated screws allow accurate fixation under fluoroscopic guidance and can provide stable fixation in selected pediatric femoral neck fractures.
Is follow-up still needed after the fracture heals?
Yes. Follow-up is important to monitor the femoral head, hip growth, limb length, and any late complications.
When can full weight-bearing start?
Weight-bearing depends on the fracture type, fixation stability, and radiographic healing. The timing should be individualized rather than generalized.
Have a hip fracture X-ray or a complex pediatric fracture?
You can send X-rays and reports by WhatsApp to determine whether clinic assessment or online review is more appropriate.
Book by WhatsApp