
This case shows the staged management of a complex knee replacement problem in a 65-year-old female patient who developed wound infection after knee replacement surgery. She underwent repeated wound cleaning/debridement procedures. During the infection-control phase, a cement spacer was used. After the wound and infection situation were controlled, the knee was reconstructed with a constrained revision knee implant, commonly referred to as an LCCK system.
Related pages
Clinical problem
Infection after knee replacement is one of the most challenging complications in joint replacement surgery. The goal is not only to treat the wound or infection, but also to preserve limb function, restore knee stability, and rebuild the joint when bone and ligament support are insufficient.
Why this was not a routine knee replacement
Revision knee replacement is technically different from primary knee replacement. In complex cases, the surgeon may need to manage bone defects, weak soft tissues, previous infection, scarred tissues, and partial loss of ligament function. A standard primary knee implant may not provide enough stability in this setting.
Treatment strategy
- Infection and wound assessment: the wound condition, inflammatory markers, cultures when indicated, and radiographs are assessed to define the safest treatment pathway.
- Debridement/cleaning stage: infected or unhealthy tissue is surgically cleaned. In staged revision cases, a cement spacer can help maintain space and alignment during the infection-control phase.
- Planning for reconstruction: bone defects, ligament competence, limb alignment, and implant fixation are reviewed carefully before definitive revision surgery.
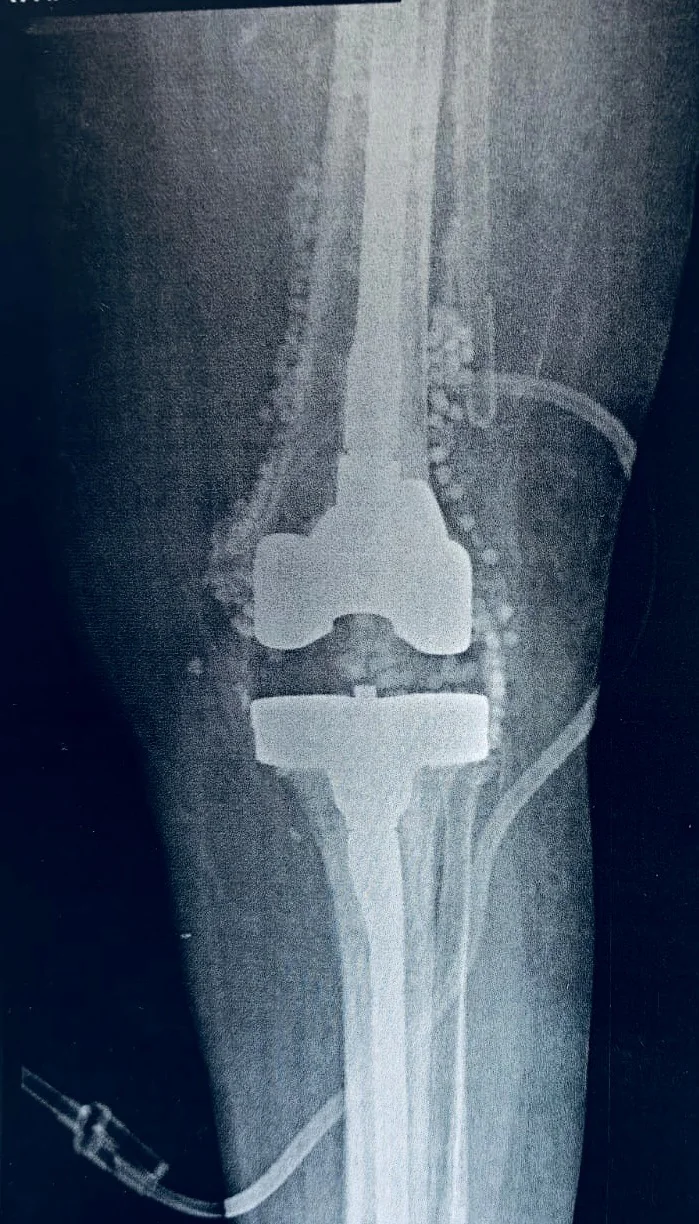
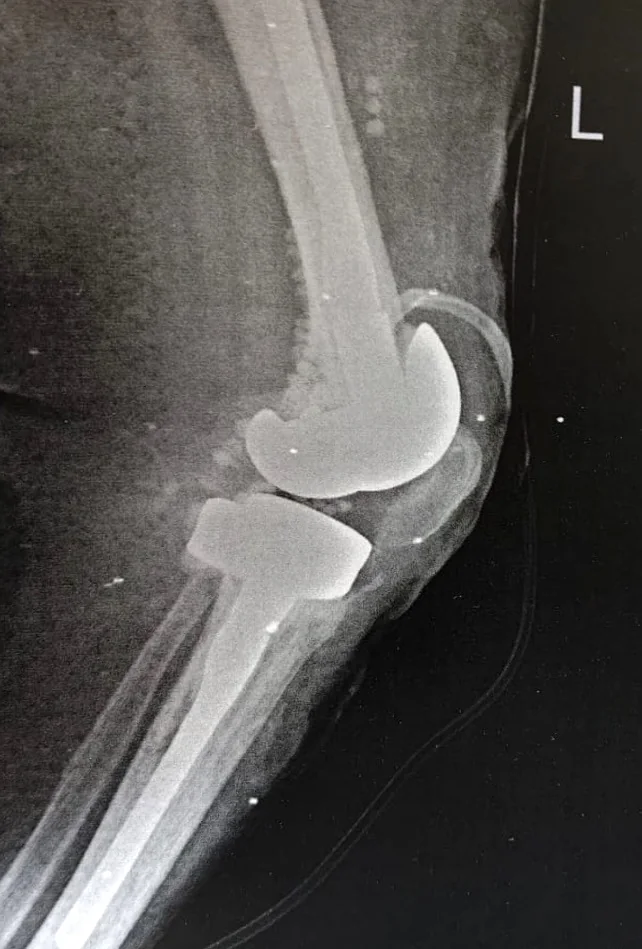
- Definitive revision knee replacement: once appropriate for reconstruction, an LCCK-type constrained revision knee implant can be used to compensate for bone loss and ligament insufficiency.
- Follow-up: revision cases require close follow-up for wound healing, infection surveillance, implant stability, physiotherapy progression, and functional recovery.
What is an LCCK revision knee implant?
LCCK refers to a constrained condylar revision knee system. This type of implant is designed for revision knee replacement cases where a standard implant may not be stable enough. It provides additional coronal-plane stability and is commonly used when there is significant bone loss, collateral ligament insufficiency, or complex revision anatomy.
- Long stems can improve fixation by transferring load into stronger bone away from the damaged joint surface.
- Constraint helps compensate for insufficient ligament support.
- The system can be combined with augments or other reconstruction options depending on the defect pattern.
Radiographic case gallery
Radiographs are shown for educational purposes only. Patient identity has been removed as much as possible before publication.


Key patient education messages
- A wound infection after knee replacement should be assessed early by a specialist in joint replacement or revision surgery.
- Repeated wound cleaning may be necessary, but persistent or deep infection can require staged reconstruction.
- A cement spacer is part of many staged strategies; it helps maintain the space for later reconstruction while treatment continues.
- Severe bone loss or ligament insufficiency may require a constrained revision implant such as an LCCK system.
- Management depends on infection control, soft-tissue healing, stable implant fixation, and structured rehabilitation.
FAQ
Is infection after knee replacement serious?
Yes. Infection after knee replacement can affect the wound, soft tissues, and sometimes the implant itself. It requires careful assessment and may need surgical cleaning, antibiotics guided by cultures, or staged revision surgery depending on severity.
Why is a cement spacer used?
A cement spacer can be used during staged treatment to maintain the joint space and limb alignment while the wound and infection problem are being managed before definitive reconstruction.
What is the role of an LCCK knee implant?
An LCCK-type constrained revision knee implant is used when the knee needs more stability than a standard implant can provide, particularly in revision cases with bone loss or deficient ligaments.
Can every infected knee replacement be treated the same way?
No. The plan depends on the duration and depth of infection, culture results, implant stability, bone stock, patient health, soft-tissue condition, and previous surgeries.
What should a patient bring for revision-knee consultation?
Previous operative reports, culture results, antibiotic history, ESR/CRP results, recent X-rays, any CT or MRI scans if available, and details of previous wound procedures are all useful.
Need a revision-knee assessment?
Complex knee replacement infection and revision surgery need individualized planning. Patients should seek specialist review if they have persistent wound discharge, recurrent swelling, increasing pain, fever, loosening, instability, or previous repeated debridement after knee replacement.
Book via WhatsApp